FRCR Part 2B (Radiology) - preparatory resources for candidates
Short case and long case reporting sample questions and responses
Before reviewing the resources below, candidates preparing for the exam should review the risr/assess demonstration site. The demonstration site includes the same questions as included below but the images will be optimised for viewing and provide better examples of the image quality in the exam. For the long case reporting sample content, the imaging for these cases is only available to view via the demonstration site.
Short case reporting sample content
Sample short cases, with an example of a good response for each, are provided below to give guidance to candidates on how to approach this component. Short, simple statements of your observations, diagnosis and recommendation are all that is needed. You do not need to write full sentences.
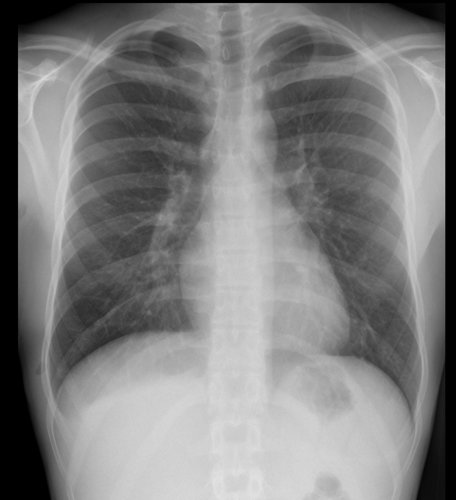
History: An 18-year-old male referred from Emergency Department with pleuritic chest pain
Findings:
Small right apical pneumothorax
Lung apex at level of posterior 2nd/3rd posterior intercostal space
No pneumomediastinum
No signs of tension
Lungs appear normal
No rib fracture
Diagnosis:
Small right apical pneumothorax
Management:
Inform ED team of finding
If patient stable, pneumothorax may resolve with conservative management
History: A 38-year-old female referred from GP with several months of tiredness and lethargy.
Findings:
Lobulated, non-calcified soft tissue mass projected over left side of mediastinum, inseparable from left heart border
Separate from left hilum (hilum overlay sign)
Mediastinum otherwise normal
Lungs and pleural spaces clear
No evidence of splenomegaly
Bones normal
Diagnosis:
Anterior mediastinal mass. Could be lymphadenopathy, thymic neoplasm or mediastinal germ cell tumour (teratoma)
Thymoma most likely, given history and lack of calcification or fat
Management:
Inform GP + 2WW referral to chest clinic
Requires CT thorax, abdomen and pelvis for further evaluation
Myaesthenia gravis screen (blood tests to identify antibody subtype)
Lung MDT discussion with view to image guided mediastinal biopsy
History: An 81-year-old male referred from GP with cough and weight loss
Findings:
Left lower lobe collapse with no visible hilar mass
Numerous calcified pleural plaques indicating previous asbestos exposure
No mediastinal lymphadenopathy
No pleural effusion
No bone metastases
Diagnosis:
Left lower lobe collapse – likely due to small central lung cancer obstructing left lower lobe bronchus in a patient with prior asbestos exposure
Mucus plugging, inhaled foreign body or endobronchial carcinoid less likely in this case
Management:
Lung MDT referral
CT chest and abdomen with IV contrast agent
Bronchoscopic biopsy likely to provide diagnosis unless CT reveals other target such as supraclavicular lymph node or liver/bone metastases
History: A 3-year-old female referred from Emergency Department with painful right elbow after fall from swing

Findings:
Fracture dislocation of right proximal radius
Displaced (avulsed) medial humeral epicondyle
No other injury seen
Management:
Inform ED staff and advise referral to fracture clinic
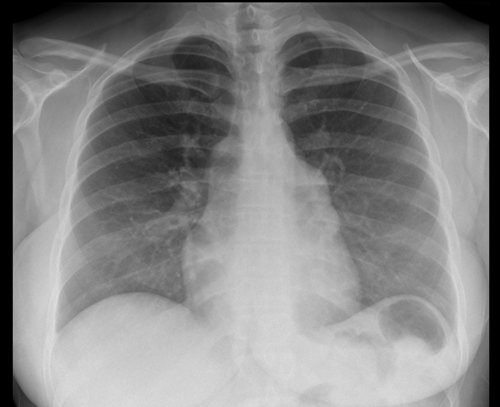
History: A 20-year-old female referred from Emergency Department with acute asthma exacerbation

Findings:
Rounded area of consolidation in left upper zone
Lungs otherwise clear
No pneumothorax or pneumomediastinum
No pleural effusion
Diagnosis:
Likely round pneumonia left upper lobe
Differential diagnosis pulmonary infarct but less likely
Management:
Inform ED staff
Suggest repeat CXR after antibiotic treatment to ensure resolution (although may not be necessary as patient is young)
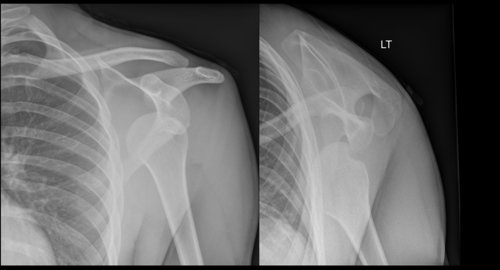
History: A 25-year-old male referred from Emergency Department with painful left shoulder after rugby injury
Findings:
Anterior dislocation of left humeral head
Bony defect in posterior humeral head (Hill Sachs impaction fracture)
Left glenoid appears intact
Acromioclavicular joint intact
No rib fracture or pneumothorax
Diagnosis:
Likely round pneumonia left upper lobe
Differential diagnosis pulmonary infarct but less likely
Management:
Suggest orthopaedic referral
May require CT or MRI shoulder after reduction for surgical planning
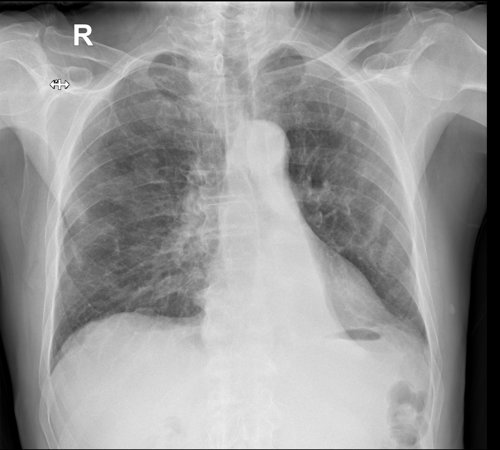
History: A 66-year-old male referred from GP with increasing shortness of breath on exertion

Findings:
Reduced lung volumes
Coarse reticulonodular opacification in both lungs, most severe at the bases
Ill-defined oval mass projected above right hilum
No mediastinal or hilar lymphadenopathy
No pleural effusions
No bony destruction
No cardiac enlargement
Diagnosis:
Likely right-sided lung cancer in patient with fibrotic interstitial lung disease (ILD)
Management:
Compare with previous imaging
2WW referral to lung MDT if patient not already under care of respiratory team
CT thorax and abdomen + IV contrast enhancement for assessment of ILD and staging of lung cancer
CT guided lung biopsy high risk due to ILD
History: A 75-year-old male referred from Emergency Department with severe hip pain

Findings:
Large, ill-defined lucency in right iliac bone extending to right sacroiliac joint medially and extending inferiorly to ischium with destruction of superior and posterior acetabulum
Wide zone of transition
No internal calcification
No other bony lesion
Diagnosis:
At this age, a bony metastasis is likely (from lung, kidney or thyroid primary). Prostatic primary less likely as not sclerotic.
Differential diagnosis multiple myeloma
Primary bone sarcoma much less likely
Management:
Urgently inform ED staff and find out whether patient has known malignancy
CT thorax, abdomen and pelvis + IV contrast enhancement for further evaluation of lesion and identification of primary cancer
Patient should be immobilised to avoid risk of pathological fracture
History: A 54-year-old female referred from GP with persistent cough

Findings:
Cystic bronchiectasis basal segments of left lower lobe
Fluid levels seen in some dilated airways, but no focal consolidation seen
Mild volume loss (depressed left hilum) likely due to recurrent mucus plugging
Cardio mediastinal contour otherwise normal
Right lung clear
Pleural spaces clear
Diagnosis:
Cystic bronchiectasis in left lower lobe
Management:
Compare with previous imaging
If no previous imaging, CT would assess extent of bronchiectasis and exclude any other pathology such as a small lung cancer
Patient may benefit from referral to respiratory clinic for ongoing management of her bronchiectasis
History: A 61-year-old female referred from GP with chest pain

Findings:
Left mastectomy and left axillary clips
Pleurally-based mass right lateral chest wall with underlying destruction of lateral aspect of right 8th rib
No other bone lesions
Lungs and pleural spaces clear
No mediastinal or hilar lymphadenopathy
Diagnosis:
Likely right 8th rib metastasis from previous breast cancer
Management:
Inform GP and make 2WW referral back to breast oncologists
Restage with CT thorax, abdomen and pelvis + IV contrast agent
If histology is needed, the rib lesion is amenable to ultrasound or CT-guided biopsy
History: A 31-year-old male referred from Emergency Department after alleged assault
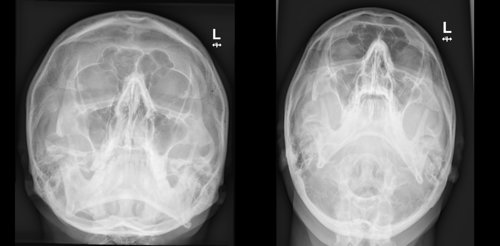
Findings:
Depressed fracture right zygomatic arch
No other bony injury
Right maxillary antrum clear
Diagnosis:
• Depressed fracture right zygomatic arch
Management:
Inform ED and recommend maxillofacial surgical referral
Many need surgical reduction (non-urgent unless associated with restriction of mouth opening due to trapping of mandibular condyle or temporalis muscle)
Consider CT to aid in surgical planning
History: A 1-month-old male referred from Neonatal Unit with abdominal distension

Findings:
NG tube tip within stomach
Numerous dilated small bowel loops
No pneumatosis or free intraperitoneal gas
Portal venous gas
Ground glass opacification at lung bases (worse on right)
Diagnosis:
Necrotising enterocolitis (NEC)
Respiratory distress syndrome (RDS)
Management:
Inform NNU staff of findings
CXR for further evaluation of lung changes
History: A 10-year-old female referred from Outpatient Clinic for follow-up imaging

Findings:
Sclerosis, flattening and irregularity of right femoral capital epiphysis
Widened right femoral neck (coxa magna)
Left femur normal
Diagnosis:
Right-sided Perthes disease (idiopathic avascular necrosis of femoral head)
Management:
Compare with previous imaging
Surgical referral (if not already under care of paediatric orthopaedic surgeons)
Consider MRI of hips to ensure no early changes on left side (15% cases are bilateral)
Long case reporting sample content
Please view the imaging for these cases on the risr/assess demonstration site. An example of a good response to each of these cases is provided below to give guidance to candidates on how to approach this component.
Observations
US abdomen – heterogenous soft tissue mass with calcifications in right suprarenal region, closely related to the liver
CT thorax and abdomen with contrast - mass adjacent to the liver likely right adrenal in origin. Internal calcifications and cystic areas.
Right adrenal not separately seen. Normal left adrenal
Mass crosses midline with encasement and displacement of major vessels including abdominal aorta and its branches.
Compressed slit-like intra-hepatic IVC.
Left supraclavicular and bilateral retroperitoneal and iliac lymphadenopathy
Bilateral iliac wing periosteal reaction and left sclerotic bone lesion
No renal mass or hydronephrosis
Small volume abdominal free fluid
A few non-specific peripheral lung lesions
Interpretation
Aggressive right adrenal/retroperitoneal malignancy
Principle diagnosis
Neuroblastoma with nodal and bony metastases
Differential diagnosis
Lymphoma less likely due to calcification
Management
Urgent referral to paediatric oncology MDT
Urinary catecholamines
MIBG scan
MRI spine
Image‑guided biopsy
Observations
Previous gastrojejunostomy
Stomach, duodenum, afferent and efferent jejunal loops dilated with transition point at level of proximal jejunum in right mid abdomen.
Well defined, gas containing intraluminal lesion at transition point
Distal small bowel and large bowel collapsed
Normal bowel wall enhancement
No free gas or free fluid
Mild fatty liver
Post cholecystectomy clips
Other solid organs unremarkable
Urinary catheter in situ
Small fat containing umbilical hernia
Minor linear atelectasis lung bases, no features of aspiration
Interpretation
See below
Principle diagnosis
Mechanical small bowel obstruction due to a bezoar (such as a phytobezoar) in the efferent limb of jejunum beyond gastrojejunostomy
Differential diagnosis
None
Management
Urgent surgical referral. Advice placement of NG tube to reduce risk of aspiration.
Possibly can be treated endoscopically rather than surgically
Observations
CT chest with contrast
Thickened interlobular septa both lungs, worst in upper zones
Bilateral ill-defined air space opacifications
Bilateral pleural effusions (right > left) with no thickening
Previous right mastectomy with enlarged axillary lymph node
Normal left axilla
No thoracic lymphadenopathy
Multiple hypodense liver lesions
Bulky left adrenal -indeterminate
Sclerotic vertebral lesions
Small hiatus hernia
Interpretation
Right axillary node, liver and bony metastases
Pulmonary features suggestive of lymphangitis carcinomatosis
Air space opacification could be due to infection or drug related pneumonitis
Principle diagnosis
Widespread metastatic breast carcinoma
Differential diagnosis
Metastases from another primary
Management
Compare with previous imaging to determine if findings are new
Right axillary node accessible for US guided biopsy if needed
Inform oncologist to raise possibility of infection and drug related pneumonitis if on chemotherapy
Video simulation of the Oral component
A role-played encounter between examiners and candidate for the FRCR Part 2B (CR2B) oral component.
Introduction to changes to the FRCR 2B Exam
FRCR 2B (Radiology) Exam Preparation Course: Tips & Techniques
Tuesday 15 September 09:00 - 17:00
Our one-day online course is designed for UK and international candidates preparing for the upcoming FRCR Part 2B (CR2B) clinical radiology exam who want to enter their assessment feeling confident and in control.
Exam information
Refer to the list of exam venues .
Instructional videos and updated exam content on the risr/assess demonstration site are available.
Following implementation of changes to the exam in June 2025 all candidates will be assessed using the new format, regardless of any previous attempts.
The type of content used in the exam is unchanged and the same minimum standards for passing the exam apply. Previous exam attempts will still count.
All candidates are advised to familiarise themselves with the new elements of the exam so that you know what to expect during the exam.
Sitting the exam
The short case reporting component will take place first, with a two-hour duration. There will be a 30-minute break before the long case reporting component will start. The long case reporting component has a 75-minute duration.
Details of timings will be provided to candidates with their individual timetables.
The risr/assess platform is used for the delivery of all CR2B components. We are happy that the image definition and manipulation features are sufficient for allowing a fair assessment of candidates’ abilities. Image quality checks are performed ahead of each sitting as part of the exam's routine quality assurance processes.
Consultant radiologists now have less exposure to plain radiographic reporting during training but will be expected to answer queries from junior radiologists or reporting radiographers for challenging cases throughout their career. Core competence in plain radiograph reporting therefore needs to undergo thorough assessment as part of the exam to ensure that residents are motivated to master this important component of departmental workload.
Resident radiologists are well aware that, for example, a ‘normal’ chest radiograph does not exclude an underlying lung cancer and that a normal appendicular radiograph does not exclude a fracture in the appropriate clinical setting, so may be reluctant to call a case normal in the absence of clinical information.
It is difficult to create a fair mark scheme for a normal case with appropriate weighting within the structure of the exam without unwittingly demonstrating to the candidate which cases are normal. Abnormal cases included in the exam all contain numerous normal anatomical structures and, as such, will also test a candidate’s ability to recognise normality.
Exclusion of normal cases allows the candidate to be assessed on a greater range of pathological conditions, thus making the assessment more robust.
Short, simple statements of your observations, diagnosis and recommendation are all that is needed. You do not need to write full sentences. Sample exam content is available.
Yes, facial bone and spinal radiographs may be included in the Short Case Reporting component and will be classified as MSK cases.
There may be congenital abnormalities. Likewise, there may be “normal variants” - however the short case is an exam of radiology pathology so in the assessment of the radiograph it is important to take into account these findings and determine their relevance by their imaging appearance and the supplied history, which should form part of the image report.
Like reporting any radiograph if there are relevant positive findings this should be part of the report/question answer.
Yes, please include this in your response, even if you are recommending no further management. Candidates should also reflect urgency if relevant to do so.
Yes, please include this in your response, even if you are recommending no further management. Candidates should also reflect urgency if relevant to do so.
If the angle is relevant to the report, then a relevant comment on the angle should be included in the question answer.
Yes, relevant pertinent negatives should be included in the report the same as they should be included in a normal radiology report.
Standardised exam content is used across each examining day. To maintain the integrity of the materials and to ensure that nobody has an unfair advantage, we must keep candidates isolated in the quarantine waiting area. Candidates must ensure that they arrive for quarantine by the time specified on their exam timetable. Candidates who arrive after this time will not be allowed entry to the exam.
Exam venues will have rooms set aside for candidates to wait before and after taking the Oral component. Whilst quarantine times may vary, all candidates should be prepared to spend most of the day at the venue. Quarantine times will be indicated on candidates’ individual timetables.
Your timetable will clearly state the time that you must be at the exam venue and details of your quarantine arrangement. You should bear this in mind when looking to make any travel arrangements.
Food, drink and study material is permitted for those in the quarantine room. No electronic devices permitted.
You will not be allowed to use electronic devices whilst being quarantined. Paper-based reading material (such as books, printed text or handwritten notes) is allowed. Candidates suspected of breaking quarantine rules will be investigated in line with the RCR’s Exam Misconduct Policy.
Candidates will be shown 12 cases across two oral sessions. All modalities in each case contribute to that one particular case and the candidate’s overall performance in that single case will be scored across the scoring domains. Individual modalities are not scored separately.
Yes, examiners will progress candidates through the cases. Examiners may move candidates onto the next case, this may be to ensure candidates have enough opportunity to view the next case or if there is no further discussion needed on that case.
No, once you have moved to the next case in the oral component it is not permitted to go back to a previous one.
If the examiners have no further questions, the session can finish early.
Yes.
Examiners have standard questions as the basis for each case but have flexibility to seek clarification of responses or ask for further detail.
Each of the examiners assessing a candidate in the oral component will provide a rating for candidate communication. This is using the same rating scale as for the other assessed domains. The communication rating is based on performance across the six cases in one oral session (rather than per case). As the communication score is assessed per oral session, it is multiplied by six to ensure it has the same weighting as the other four skill domains.
Examiners will have access to question-specific marking schemes for each case.
The oral component is marked by the pair of examiners conducting each session. Scores from all examiners (across both stations) are then totalled.
All Short Case and Long Case questions are independently double marked and scores from both examiners contribute to your total final score.
See the scoring system for more details.
After the exam
All candidates will receive a pass/fail notification with a breakdown of their scores across the three components and standardised feedback. As candidates will be provided with all available details of their performance across each component, no further information will be provided.
As the oral component is delivered using the risr/assess platform, all marking is captured within the platform and no marking retained in paper-based marksheets.
Specific result release dates will be added on the website for each exam sitting. Ordinarily results will be available within four weeks after the exam week.
Yes. This can be awarded to an outstanding candidate on recommendation of the Examining Board, based on performance, at each sitting of the exam
An initial pass mark for the oral component has been determined (via the Ebel/Angoff standard setting methodology). A post exam review is conducted to ensure consistency and fairness to candidates. This may result in adjustment to the oral pass mark for a particular day of the orals. Information on the pass mark for this component is included in the information sent to candidates following their exam.
You will receive a breakdown of your scores across the three CR2B components. If you receive a zero score for a question or specific domain this means the examiners have allocated a zero score. It does not relate to a missing mark. A number of checks are conducted to ensure that all marking is complete and no marks are missing. You can find more information on the scoring scales used in the CR2B scoring system information.
A thorough post-exam review is conducted to ensure consistency of standards and fairness to candidates whilst upholding patient safety. This may result in the removal of individual questions from the score calculation. Decisions on question removal are taken by an expert panel and with consideration to the question performance and question content. If a decision is made to remove a question, there is a review to ensure that the remaining content still represents appropriate content coverage and exam metrics remain robust and fair. When a flawed question is removed from an exam, candidates are not penalised. This is because a question that doesn’t reliably distinguish between stronger and weaker performance introduces random error rather than meaningful assessment. Removing such a question helps ensure that everyone’s final score is a fairer and more accurate reflection of their true competence.