Short case reporting sample content
Case 1 (CXR)
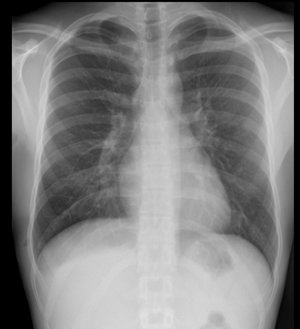
History: An 18-year-old male referred from Emergency Department with pleuritic chest pain
Findings:
Small right apical pneumothorax
Lung apex at level of posterior 2nd/3rd posterior intercostal space
No pneumomediastinum
No signs of tension
Lungs appear normal
No rib fracture
Diagnosis:
Small right apical pneumothorax
Management:
Inform ED team of finding
If patient stable, pneumothorax may resolve with conservative management
Case 2 (CXR)
History: A 38-year-old female referred from GP with several months of tiredness and lethargy.
Findings:
Lobulated, non-calcified soft tissue mass projected over left side of mediastinum, inseparable from left heart border
Separate from left hilum (hilum overlay sign)
Mediastinum otherwise normal
Lungs and pleural spaces clear
No evidence of splenomegaly
Bones normal
Diagnosis:
Anterior mediastinal mass. Could be lymphadenopathy, thymic neoplasm or mediastinal germ cell tumour (teratoma)
Thymoma most likely, given history and lack of calcification or fat
Management:
Inform GP + 2WW referral to chest clinic
Requires CT thorax, abdomen and pelvis for further evaluation
Myaesthenia gravis screen (blood tests to identify antibody subtype)
Lung MDT discussion with view to image guided mediastinal biopsy

Case 3 (CXR)
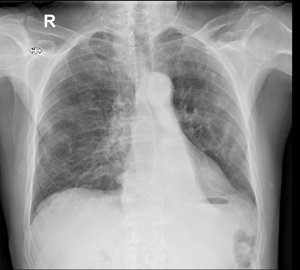
History: An 81-year-old male referred from GP with cough and weight loss
Findings:
Left lower lobe collapse with no visible hilar mass
Numerous calcified pleural plaques indicating previous asbestos exposure
No mediastinal lymphadenopathy
No pleural effusion
No bone metastases
Diagnosis:
Left lower lobe collapse – likely due to small central lung cancer obstructing left lower lobe bronchus in a patient with prior asbestos exposure
Mucus plugging, inhaled foreign body or endobronchial carcinoid less likely in this case
Management:
Lung MDT referral
CT chest and abdomen with IV contrast agent
Bronchoscopic biopsy likely to provide diagnosis unless CT reveals other target such as supraclavicular lymph node or liver/bone metastases
Case 4 (XR Right Elbow)
History: A 3-year-old female referred from Emergency Department with painful right elbow after fall from swing
Findings:
Fracture dislocation of right proximal radius
Displaced (avulsed) medial humeral epicondyle
No other injury seen
Management:
Inform ED staff and advise referral to fracture clinic

Case 5 (CXR)
History: A 20-year-old female referred from Emergency Department with acute asthma exacerbation
Findings:
Rounded area of consolidation in left upper zone
Lungs otherwise clear
No pneumothorax or pneumomediastinum
No pleural effusion
Diagnosis:
Likely round pneumonia left upper lobe
Differential diagnosis pulmonary infarct but less likely
Management:
Inform ED staff
Suggest repeat CXR after antibiotic treatment to ensure resolution (although may not be necessary as patient is young)

Case 6 (CXR)
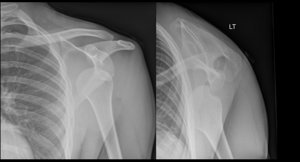
History: A 25-year-old male referred from Emergency Department with painful left shoulder after rugby injury
Findings:
Anterior dislocation of left humeral head
Bony defect in posterior humeral head (Hill Sachs impaction fracture)
Left glenoid appears intact
Acromioclavicular joint intact
No rib fracture or pneumothorax
Diagnosis:
Likely round pneumonia left upper lobe
Differential diagnosis pulmonary infarct but less likely
Management:
Suggest orthopaedic referral
May require CT or MRI shoulder after reduction for surgical planning