‘Alarm bells should be ringing’: staff shortages causing ‘extremely dangerous’ delays to diagnosis and cancer care, doctors warn
A worsening shortage of radiologists and cancer doctors is causing dangerous delays to diagnosis and treatment for patients across the UK, according to new Royal College of Radiologists (RCR) 2025 workforce data.
The RCR warns that without action to boost the workforce, more patients will suffer as demand continues to rise. The reports give an authoritative picture of UK diagnostic and cancer services, based on responses from 100% of UK cancer centre and radiology department leaders.
Key findings:
8 in 10 radiology leaders and half of cancer leaders say staff shortages are causing patients’ conditions to worsen
Severe shortages of radiologists and cancer doctors are driving delays to diagnosis and treatment of cancer and other serious conditions
Workforce shortages are worse in deprived and rural areas
Recruitment freezes affecting radiology departments and cancer centres have doubled in a year
The government must expand training and end recruitment freezes to prevent delays worsening further
The reports reveal concerning new insights:
Staff shortages harming patients, delaying cancer treatment, and hampering government ambitions to improve cancer care
For the first time, 8 in 10 UK radiology leaders and half of cancer leaders say they have seen patients’ conditions worsen as a result of staff shortages.
9 in 10 cancer leaders have seen delays to patients starting radiotherapy or drug-based treatment including chemotherapy as a result of staff shortages.
Meanwhile, diagnostic wait and cancer treatment targets continue to be missed. NHS England data show that in 2025, nearly a million (940,900) scan results took longer than the target of a month. In 2025, only 69% of patients started cancer treatment within 62 days of a referral, against a target of 85%. Just 40% started radiotherapy within the same timeframe.
Delayed diagnosis leads to delayed treatment and can worsen health outcomes – particularly for people with cancer, where every month’s delay to starting treatment can increase the risk of death by around 10%.
“[Staff shortages are causing] delays in patients starting both chemotherapy and radiotherapy treatment.” – cancer centre leader
“Workforce shortages in diagnostics especially radiology and pathology are critical and lengthening pathways which is leading to patient harm.” – cancer centre leader
“Significant delays in [scan] acquisition and reporting of a wide range of patients have negatively impacted prognosis, potential treatment options and resulted in harm.”– radiology clinical director
Staff shortages are getting worse
A longstanding failure to train up enough new doctors has led to chronic workforce shortages. The UK has 32% (over 2,300) fewer radiologists and 17% (over 230) fewer clinical oncologists than it needs just to meet current demand. These workforce shortfalls have risen since 2024, from 29% to 32% for radiologists and 15% to 17% for clinical oncologists. Shortages will rise to 40% (over 4,050) too few radiologists and 26% (over 450) too few clinical oncologists by 2030 if no action is taken to boost the workforce.
“We get constant communications from referrers about patients worsening while they are either waiting for scans or reports. Memory clinic won't see new patients without a scan, and they are all stuck on our waiting list (some for almost a year!), with worsening symptoms. We are failing to meet the NHSE targets regularly.” – radiology clinical director
Demand is outpacing supply
Demand for scans is growing at more than twice the rate of radiologists to interpret them, and cancer incidence is rising. Meanwhile, nearly half (44%) of clinical oncologists and 2 in 5 (39%) radiologists are set to retire within 10 years.
“20% of our clinical oncology consultants are due to retire in the next 2 years, which presents a significant concern with staffing.” – cancer centre leader
Stark geographic divide in staffing of diagnostic and cancer services
For the first time, the RCR reports reveal a stark geographic divide in staffing that is exacerbating existing inequalities.
The shortage of clinical oncologists in deprived areas and rural communities is 2x higher than in less deprived communities and urban areas. This means that patients could face longer waits to get the cancer treatment they need. In some areas, patients may also need to travel further to access specialist treatment.
The shortage of radiologists is much worse in small acute hospitals (43% shortfall) than in large teaching hospitals (30% shortfall). The North of Scotland, North and West Wales, and the North East and East Midlands in England have some of the worst shortages.
Recruitment freezes double despite staff shortages and patient delays
Recruitment freezes stopping hospitals from hiring the radiologists and oncologists they need have doubled in a year, despite chronic shortages of these doctors causing widespread delays for patients. In 2025, 38% of radiology departments and 51% of cancer centres experienced a recruitment freeze, up from 19% and 23% respectively in 2024.
Recruitment freezes are making it harder to hire the doctors we need, particularly in areas that need them most. Cancer centres in deprived areas and rural communities have 2x higher workforce shortages, yet 60% had recruitment freezes in 2025, versus 48% in less deprived areas and urban communities.
Bans on hiring permanent staff are a false economy. They force trusts and health boards to fill the gaps with expensive outsourcing, locums, and overtime. They are a direct blocker to delivering safe, effective patient care, leading to staff burnout, retention challenges, and discontinuity of care.
“There is an effective freeze on retention and recruitment of all staff ...I am concerned that, even though the trust has prioritised cancer performance, they fail to understand that supporting CT, in particular, and recruiting the radiologists to report the scans, attend multidisciplinary team meetings, and do the biopsies are essential if we wish to improve our cancer performance.” – radiology clinical director
“Recruitment freeze and removal of 25% of radiography and physics posts has directly resulted in a 10-week waiting time for radiotherapy.” – cancer centre leader
The NHS is spending record sums on short-term fixes to fill workforce gaps while failing to address the root cause
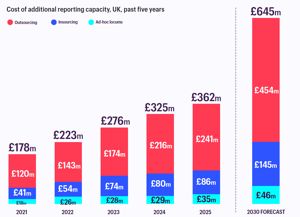
In radiology, the UK spent a record £362 million in 2025 on outsourcing, paid overtime, and locums – enough to pay over 3,000 radiology consultant salaries, far more than the current shortage of 2,300. Outsourcing scans to be read by private companies accounted for £241 million of this cost; this expense is on track to rise to £454 million by 2030.
This chart shows the soaring cost of the shortage of radiologists.
We must reduce reliance on outsourcing. 86% of radiology leaders are concerned about the quality of outsourced reports, and 90% are concerned they need double-checking, adding to their teams’ packed workloads and delaying patients’ scan results. Many radiology leaders are concerned this does not represent good value for money.
“Workforce shortages delay report turnaround time, impacting on patient care. Increasingly, the shortfall is met with outsourcing which reduces quality of patient reports and increases pressure on local radiologists for second review.” – radiology clinical director
Recommendations for government action:
Instead of haemorrhaging money on short-term fixes, governments must:
Invest in training more doctors by increasing the number of training places for clinical radiology and clinical oncology. This would save £120 million compared to short-term fixes.
In 2025, the NHS spent a record £362 million on temporary solutions to fill the radiology workforce gap, enough to fund over 3,000 radiology consultant salaries – more than the entire shortfall.
Modelling commissioned by the RCR shows that training up just 10% more radiologists per year would save the NHS £100 million, compared to relying on short-term fixes like outsourcing, and create half the radiologists we currently need, after 10 years. Radiology training posts are increasingly competitive, so there is no shortage of resident doctors keen to train as radiologists.
Adding just 10 extra clinical oncology training posts per year would, after 10 years, eliminate the shortage of these doctors and save the NHS approximately £20 million.
Scrap recruitment freezes imposed on radiology departments and cancer centres.
This short-sighted cost-cutting measure is a direct blocker to delivering safe, effective care, and yet recruitment freezes have doubled in a year while staff shortages have risen.
Freezes must be scrapped, through intervention by national NHS leaders where necessary.
Maximise training capacity by allocating training places by whole-time equivalent (WTE) rather than by headcount.
Capacity to train more clinical radiologists and clinical oncologists should be maximised by allocating training posts by WTE instead of by headcount.
If a trainee who works part-time were counted as ‘0.6’ WTE instead of ‘1’ training post, for example, the remaining ‘0.4’ funding could be reallocated to another trainee, providing more training posts in total with the same amount of funding.
Quote from RCR spokesperson:
Dr Stephen Harden, President of the Royal College of Radiologists, said:
“For the first time, our census shows that patients’ conditions are deteriorating because of workforce shortages. Delays to diagnosis and cancer treatment are extremely dangerous, particularly in deprived and rural communities where shortages are worst.
Despite our members’ extraordinary efforts, we simply don’t have enough clinical radiologists and clinical oncologists to meet rising demand. Recruitment freezes and growing reliance on outsourcing are making the situation worse not better.
Alarm bells should be ringing for governments across the UK. Without urgent action to train, recruit and retain more doctors, more patients will suffer.”
Quote from patient case study:
Jenny, 51, is an Assistant Headteacher from Hull, living with stage 4 bowel cancer. She said:
“Waiting for scan results is one of the worst parts of living with cancer and has a severe impact on my mental health. I’ve waited up to 5 weeks for results before. It’s just not good enough – I shouldn’t have to suffer that long in fear, on autopilot, not knowing what my future looks like. I can tell that staff are overworked and burnt out. How are we so advanced in some ways and yet so backwards when it comes to timely care?”
Quotes from spokespeople across the health sector:
Matt Sample, senior health policy manager at Cancer Research UK, said:
"Having enough radiologists and oncologists is vital for ensuring people affected by cancer are diagnosed and treated quickly. But right now, workforce shortages mean that every month, thousands of cancer patients across England are waiting longer than they should to begin their treatment. It's particularly concerning that so many specialists have reported seeing patients' conditions worsen as a result of staff shortages.
"The UK Government needs to tackle this problem with its upcoming 10-year workforce plan which must provide investment for more specialist staff so that cancer patients can get timely diagnoses and treatment. Without this, people affected by cancer will continue to be let down."
Genevieve Edwards, Chief Executive at Bowel Cancer UK, said:
“Behind every delayed test result is a real person lying awake at 3am waiting for news that could change everything.
Too many people affected by bowel cancer are already waiting far too long for tests, scans and answers, and workforce shortages are making it worse. That weight of uncertainty is something no one should have to carry longer than necessary.
With bowel cancer, finding it early can make a real difference to treatment options and survival. That's why we urgently need to train and recruit more staff so patients can get the tests, results and care they need without unnecessary delays.”
Melanie Sturtevant, Associate Director of Policy, Evidence and Influencing at Breast Cancer Now , said:
“Early diagnosis and prompt treatment are critical to give people with breast cancer the best chance of survival, and delays can have devastating consequences.
With a significant proportion of the specialist breast cancer workforce approaching retirement within 5 years, urgent action must be taken to stop the situation deteriorating further.
NHS staff are working tirelessly under intense pressure, but they cannot continue to deliver the care patients need without workforce capacity that matches rising demand.
The imminent NHS Workforce Plan for England must invest in growing, retaining and supporting the cancer workforce. Only then can we ensure people with breast cancer access fast, high-quality treatment and care.”
Craig Jones, Chief Executive of the Royal Osteoporosis Society , said:
“Radiologists play a vital role in diagnosing osteoporosis and identifying fractures, so it is deeply concerning to see the scale of workforce shortages set out in this report. Delays to scan interpretation and diagnosis can leave patients living with pain and uncertainty for far too long and can mean opportunities to prevent further fractures are missed.
Osteoporosis is often described as a silent condition because many people do not realise they have it until they break a bone. Timely access to scans, rapid interpretation of results and clear follow-up care are all essential if patients are to receive the treatment and support they need.
The Government has committed to roll out Fracture Liaison Services to every part of England, a policy that now needs an implementation timetable to remain credible. Radiology capacity is an important part of the picture.”
Notes to editors
Media contact: [email protected] +442038054065
All statistics, unless otherwise stated, come from the Royal
College of Radiologists (RCR) reports, published on 18th June 2026:
These annual reports are based on survey responses from 100% of the UK’s cancer centre heads of service and clinical directors of radiology departments. They are an authoritative source of information about the state of diagnostics and cancer care in the UK. Running since 2008, they identify trends and make evidence-based recommendations.
The Royal College of Radiologists is the leading professional membership body for clinical radiologists and clinical oncologists.
Clinical radiologists are specialist doctors who use imaging to diagnose, monitor and treat diseases and injuries. They are experts in interpreting medical imaging including CT and MRI scans, and delivering image-guided minimally invasive procedures, including stroke treatment. They are responsible for the majority of diagnoses made in the NHS.
Clinical oncologists are specialist doctors who manage cancer. They prescribe, plan, and oversee delivery of drug-based treatments, such as chemotherapy, and radiotherapy.
‘Deprived areas’ refers to deprived population in England, as defined as cancer centres that serve Integrated Care Boards (ICBs) in the bottom 25% of the English indices of deprivation rankings.
‘Rural communities’ refers to the cancer centres in Scotland, Wales, and Northern Ireland that serve the most rural or remote catchment population.
Where this press release refers to ‘smaller’ and ‘larger’ hospitals, trust/health board size has been determined by the number of consultant clinical radiologists (whole-time equivalent) employed in 2025. The 25% with the most are ‘large’ and the 25% with the fewest are ‘small’.