AI underused where it could deliver significant productivity gains, says RCR
New 2025 UK workforce data from the Royal College of Radiologists (RCR) show that while AI use is growing rapidly in UK diagnostics and cancer care, it is being underused in administrative tasks where it could have significant untapped potential to ease workload pressures.
Radiology: AI underused in admin where it reduces workload the most
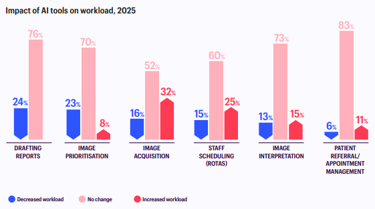
75% of radiology departments now use AI, up from 69% in 2024. The most common use is to help radiologists identify features of interest when analysing scans, with 58% of departments using AI in this way.
However, far fewer are using AI for admin tasks. Only 13% of departments use AI for staff scheduling and rotas, 12% for managing patient referrals and appointments, and 11% for report drafting. Yet, AI for report drafting delivers the biggest benefit: nearly a quarter (24%) of radiology departments using AI in this way say it reduces workload – the highest of any AI use case in radiology.
These findings suggest AI could have considerable untapped potential to increase productivity if it were used more widely for administrative tasks alongside clinical applications. Radiologists spend significant time on admin, so expanding the use of AI in this area could help reduce workload pressure and free up more time for patient care. The NHS should focus on implementing effective AI tools for admin tasks.
Despite increasing adoption, implementing, monitoring and evaluating AI takes time, expertise and sufficient staffing. The 2025 data suggest that AI is not yet reducing radiologists’ workloads overall.
Oncology: AI reduces treatment planning workload, but also has significant potential in admin
According to the 2025 data, 81% of cancer centres are now using AI for at least one purpose, up from 63% in 2024.
During 2025, 66% of cancer centres implemented some form of AI, and 84% of those reported a positive impact.
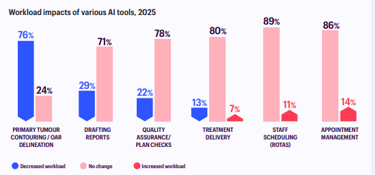
The most common use of AI to plan radiotherapy treatment, used by 81% of cancer centres. This involves AI outlining tumours and organs on medical images to show where treatment should be targeted, which are then checked by an oncologist, saving them time. Three quarters (76%) of cancer centres using AI in treatment planning say it reduces their workload – a huge productivity gain.
However, as in radiology, admin uses of AI remain underdeveloped. Only 26% of cancer centres are using AI for drafting reports, but 29% of those say it reduces workload - a significant positive impact that is not yet being realised at scale.
The NHS should ensure all cancer centres have access to AI for radiotherapy treatment planning and focus on implementing effective AI tools for admin tasks in oncology.
Dr Stephen Harden, President of the RCR, said:
“Our findings make clear that AI has significant potential to help doctors manage rising demand, but its implementation in diagnostic and cancer services must be led by evidence.
The NHS has begun introducing AI tools for administrative tasks, but these findings suggest there is considerable scope to expand their use where they can have a positive impact on productivity. AI does not mean we need fewer doctors. In fact, the UK is short of 2,300 clinical radiologists and 230 clinical oncologists needed just to meet current demand, with shortages set to worsen amid soaring demand for scans and cancer care. AI will deliver its greatest benefits for patients when we have the workforce, infrastructure and clinical oversight needed to implement it safely and effectively.
We will continue to work closely with policymakers to develop strong regulation that keeps patients safe when AI is used in their care.
But the reality is that AI is developing at such a pace that hospital teams need more help to maximise the benefits and minimise the risks. Alongside regulation, clinicians and NHS organisations need practical guidance on selecting, implementing and monitoring AI safely in day-to-day practice. We look forward to continuing to work closely with the NHS to develop this.”
Notes to editors
Media contact: [email protected] +442038054065
The Royal College of Radiologists (RCR) is the leading professional membership body for clinical radiologists and clinical oncologists.
Clinical radiologists are specialist doctors who use imaging to diagnose, monitor and treat diseases and injuries. They are experts in interpreting medical imaging including CT and MRI scans, and delivering image-guided minimally invasive procedures, including stroke treatment. They are responsible for most diagnoses made in the NHS.
Clinical oncologists are specialist doctors who manage cancer. They prescribe, plan, and oversee delivery of drug-based treatments such as chemotherapy and radiotherapy.
The RCR 2025 Clinical Radiology and Clinical Oncology Workforce Census reports were published on 18th June 2026. These annual reports are based on survey responses from 100% of the UK’s cancer centre heads of service and clinical directors of radiology departments. They are an authoritative source of information about the state of diagnostics and cancer care in the UK. Running since 2008, they identify trends and make evidence-based recommendations.
The RCR Global AI Conference 2026 - Human + machine: clinician-led AI for tomorrow's healthcare takes place from 29-30th June 2026, at the QEII Centre in London and online.